Blog Series: The Basic Breakdown of Orthopedic Injuries - Your Knee (Part 1)
Welcome to my blog series highlighting each joint one by one! Right off the bat, I would like to provide a caveat...while I will be working through each body part/joint individually, it is so important to remember that our body truly does work together to form a whole. You are not just a knee or a shoulder or a spine...you are the sum of your parts, and ALL of your parts play a role in your overall well-being! I tell you this because in physical therapy, we like to look at you as a whole person. Many things physically can contribute to knee pain (ie. you may have a torn knee ligament, but there could have been core and hip weakness that predisposed you to such an injury). Likewise, some types of pain can often be tied back to other things that are going on in your life (or have happened in the past), both physically and emotionally. Stress, for example, can wreak havoc on your body (again both physically and emotionally!). Tip #1: You are not a knee or a shoulder. You are a whole person. Be sure to take care of all of you (and find a PT who will do the same!).
Last week I gave you a brief overview of some basic anatomy, highlighting different types of structures and tissue within your body. If you haven’t read that and would like to, click here. This week I will start our journey of the orthopedic body at the knee. The knee is a common area that we see in physical therapy for a variety of reasons. It seems like a perfect place to start. Today is Part 1 of the knee, covering primarily the structure of the knee. Stay tuned for Part 2, which will cover more about the function of the knee, a few more common injuries, and a few preventive exercises and tips!

The Knee Joint Structure
Bone Structure - The knee joint is the largest joint in the human body. It is mostly considered a “hinge joint”, in that it hinges forward and back much like a door opens and closes. The knee is located at the ends of the femur and tibia bones that act as long lever arms to bend and straighten it. Because of its location and function, the knee joint is fairly susceptible to injury both from trauma and from repetitive use. In addition to the femur and tibia at the knee joint, you will also find the fibula and the patella (or the knee cap) bones. The patella sits on top of your knee and glides within a groove at the joint to allow for smooth motion (put your hand on top of your relaxed and mostly straight knee and wiggle the knee cap around to get a feel for how it “floats” above your knee).
Ligaments and Cartilage - Your knee is well-stabilized by not only the dynamic muscles surrounding it but also by four ligaments within it. The anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL) help to stabilize the joint from the back to front and the front to back. The medial and lateral collateral ligaments (MCL and LCL) help stabilize the knee side to side. The ACL and MCL ligaments are at a higher risk of being injured during physical activity due to the longer lever arms mentioned above, structural stress at the joints and/or blunt force to the knee. Oftentimes, tears of these ligaments need to be surgically reconstructed, as they are very important stabilizers of the knee over the course of our lives.
In addition to the ligaments, the knee joint is lined with articular cartilage at the ends of the bones themselves to allow for cushion and smooth gliding of the joint. The knee has extra areas of something called fibrocartilage sitting on top of the lower tibia bone, individually known as a meniscus. There are two menisci at the knee, one on the inside and one on the outside of the knee. The planting and twisting nature of your foot on the ground as you walk, turn, squat, etc, increases the risk of injury to this layer of cartilage of the knee. The medial (inside) meniscus is injured more often than the lateral (outside) meniscus because of the postural stress and the body’s natural movement patterns. Some research has shown that many meniscus tears do as well with conservative treatment (meaning rest, physical therapy, etc.) as they do with surgical intervention. Either way a meniscal injury may speed up the onset of some arthritis at the knee, as the natural cushioning of the knee is disrupted.

Muscles - There are a few muscles that cross the knee joint and help control the knee. Your quadriceps are the long muscles on top of your thigh that run from your hip/pelvis down to cross the knee. The “quads” consist of four muscles called the rectus femoris, vastus medialis, vastus intermedius, and the vastus lateralis. As a therapist, we are able to identify what muscles may be causing tightness, weakness, pulling of the patella, etc. when we look at your injury/pain upon evaluation. The quadriceps muscles help to straighten the knee when it is bent. They also contract while standing or moving to give the knee stability and keep it straight, keep it from buckling, and help control it while bending the knee when your foot is planted on the ground (lots of complexities here, with different ways that a muscle can actually function!).
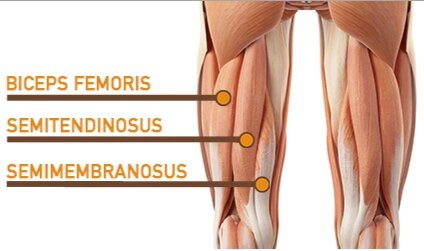
The next large muscle group at the knee is called the hamstrings. Your hamstrings run from the back of the hip/pelvis down the length of your thigh and cross the knee at the back of the joint. Again at the hamstrings there are multiple muscles to consider. They are called the semimembranosus and semitendinosus (on the inside) and the biceps femoris (on the outside). These muscles help to bend the knee when it is straight and also provide control to the hip and knee when you are up moving around, going up and down stairs, etc.
Another larger muscle that crosses the knee joint is called the gastrocnemius or the large calf muscle. This muscle starts just above the knee in the back and runs down the back of the lower leg to attach at the back of the heel. While it mostly controls movement at the ankle, it is relevant because it does cross the knee joint.
The last muscle I will touch on for the knee is actually a combined muscle/connective tissue complex that tends to sometimes be a painful structure due to its connections. It is called the tensor fascia lata (TFL) muscle + iliotibial band (often known as the IT band or ITB). The TFL is a small muscle up by the hip that generally assists some of the bigger hip muscles to move and stabilize at the hip, but it’s attachment to the IT band of connective tissue down the outside of the thigh makes it quite relevant to your knee. The ITB actually attaches itself to the outside or lateral part of the knee and can affect the movement of the patella as you bend and straighten your knee. Therefore, this TFL/ITB structures are of importance in evaluating your injury or knee pain.
As you can see, the knee has lots of important moving parts and pieces! To avoid this blog going on forever, check back soon for Part 2 of my knee coverage! Next up will be more on how the knee functions, some common injuries and some words on how to keep your knee healthy as you navigate your daily life. Do you have knee pain and think it might be wise to have a chat with me? Click here to schedule your physical therapy evaluation or a free consult call! (Must reside in the Leander and Cedar Park, Texas areas to schedule!)
Enjoy your day!
Xo,
Jill